Voice
Definition
According to the state of Minnesota, a voice disorder refers to the absence of voice or presence of abnormal quality, pitch, resonance, loudness, or duration. Voice patterns that can be attributed only to dialectical, cultural, or ethnic differences or to the influence of a foreign language must not be identified as a disorder.
Eligibility Criteria
The following criteria are taken from the Minnesota Department of Education and Legislature (Minnesota Revisor, 2007).
A student has a voice disorder and is eligible for speech or language special education when:
- the pattern interferes with communication as determined by an educational speech language pathologist and either another adult or the student; and
- achievement of a moderate to severe vocal severity rating is demonstrated on a voice evaluation profile administered on two separate occasions, two weeks apart, at different times of the day.
Characteristics
The following information regarding the characteristics of voice disorders was taken and adapted from ASHA.
- An organic voice disorder is physiological and results from changes in respiratory, laryngeal, or vocal tract mechanisms. It can be either:
- o Structural: Comes from physical changes in the vocal mechanism such as changes in vocal fold tissues (e.g., edema or vocal nodules) and/or structural changes in the larynx due to aging
- o Neurogenic: Comes from problems with the central or peripheral nervous system innervation to the larynx that affect functioning of the vocal mechanism such as a vocal tremor, spasmodic dysphonia, or vocal fold paralysis.
- A functional voice disorder is caused by inefficient use of the vocal mechanism when the physical structure is normal such as vocal fatigue, muscle tension dysphonia, or aphonia.
When someone is perceived to have symptoms of a voice disorder, it may be referred to as dysphonia. Dysphonia is characterized by a change in vocal quality, pitch, loudness, or vocal effort. These are some of the symptoms you might notice in students with dysphonia:
- Rough vocal quality (raspy, audible aperiodicity in sound)
- Breathy vocal quality (audible air escape in the sound signal or bursts of breathiness)
- Strained vocal quality (increased effort; tense or harsh)
- Strangled vocal quality (as if talking with breath held)
- Abnormal pitch (too high, too low, pitch breaks, decreased pitch range)
- Abnormal loudness/volume (too high, too low, decreased range, unsteady volume)
- Abnormal resonance (hypernasal, hyponasal, cul-de-sac resonance)
- Aphonia (loss of voice)
- Phonation breaks
- Asthenia (weak voice)
- Gurgly/wet-sounding voice
- Pulsed voice (fry register, audible creaks, or pulses in sound)
- Shrill voice (high, piercing sound, as if stifling a scream)
- Tremorous voice (shaky voice; rhythmic pitch, and loudness undulations)
- Frequent coughing or throat clearing (may worsen with increased voice use)
- Excessive throat or laryngeal tension/pain/tenderness
The perception of the student’s voice quality can vary, depending on the type and severity of the disorder, size and site of the lesion (if present), and the individual’s compensation. The severity of the voice disorder cannot always be determined by auditory-perceptual voice quality alone. Therefore, further instrumental assessment may be needed to determine the severity and/or etiology of a voice disorder. The speech-language pathologist may ask the family to follow up with their primary care doctor to obtain a referral for a medical examination regarding the voice concerns.
Causes/Etiology
The following information regarding the causes of voice disorders was taken and adapted from ASHA.
Structural
- A voice disorder may be caused by structural issues, including:
- o Vocal fold abnormalities such as vocal nodules, cysts, polyps, edema or glottal stenosis
- o Inflammation of the larynx due to issues such as laryngitis, or laryngopharyngeal reflux
- o Trauma to the larynx such as intubation trauma, chemical exposure, or external trauma
Neurological
- Voice disorders can be caused by neurological conditions such as:
- o Recurrent laryngeal nerve paralysis
- o Adductor/abductor spasmodic dysphonia
- o Parkinson’s disease
- o Multiple sclerosis
- o Pseudobulbar palsy
Trauma
- Voice disorders can also be caused by phonotrauma, which includes yelling, screaming, excessive throat clearing/coughing and speaking in too high or low of a pitch. This may also include vocal fatigue due to overuse.
Psychogenic
- There are also psychogenic causes of voice disorders, including chronic stress disorders, anxiety, and depression.
Team Interventions and Support
A whole team approach to managing a student’s voice disorder is essential. The following are recommendations for ensuring proper management at school and home.
- A referral to an Ear, Nose and Throat Specialist (ENT) may be necessary to determine whether the vocal cords have any medical reason for the voice difficulties (e.g., nodules, polyps).
- Educate the family and people in the child’s educational setting about the nature of the voice difficulty.
- Educate the family and child about how voice is produced and how damage can occur to the vocal cords.
- Practice specific exercises, techniques, and strategies on how to use the voice effectively.
- Stay hydrated.
- Teach strategies such as hitting a pillow when angry rather than screaming and shouting.
- Reduce loud shouting in play or regular conversation. Many schools have voice volume charts such as the following that can help students regulate their voice volume more effectively.
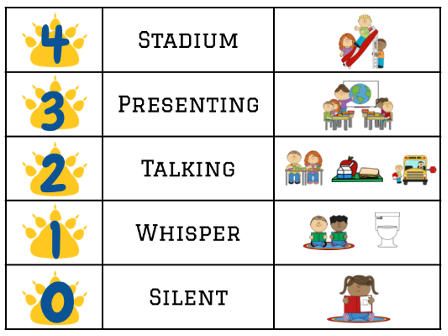 Note. From North Woods Elementary (Wayzata Public Schools).
Note. From North Woods Elementary (Wayzata Public Schools).